




- Privacy Policy
- Terms & Conditions
- Contact us
- ©Isabel Healthcare 2025
June 4, 2012




The Isabel Healthcare 1 Minute Read program highlights various diseases and conditions, providing the Isabel tool differential list. Subscribe to the Isabel blog to receive clinical content and articles.
Dyspnea (synonyms: shortness of breath, dyspneic, dyspnoeic, dyspnea, SOB, breathlessness) is a feeling of difficulty in breathing or labored breathing which is out of proportion compared to the person’s level of activity.
People with dyspnea experience an increased effort to move the chest muscles and allow adequate oxygenation. This leads to panicky feelings of being smothered and also feelings of chest wall cramping. Anxiety can heighten these feelings as people struggle to breathe.
The feeling of breathlessness is caused by several mechanisms which include increased work of breathing and therefore increased receptor stimulation in the airways, lung parenchyma, chest wall and excessive stimulation of the respiratory centre by chemoreceptors. These stimuli are then transferred to the central nervous system via the respiratory muscles which results in breathing difficulty.
A patient presenting with dyspnea could have a wide array of diseases ranging from self-limiting ones to urgent life-threatening conditions which can involve many systems of the body. The key to managing a patient with dyspnea is to thoroughly evaluate the clinical presentation, the patient’s past medical history, the physical examination and any preliminary test results which are available.
It is very important that any patient presenting with dyspnea that the clinician makes a rapid assessment of the airway and ensures it’s secure. This should be done by positioning the patient to maintain the airway, obtain pulse oximetry readings and associated arterial blood gases and provide supplemental oxygen as required.
Once the Airway, Breathing and Circulation has been evaluated and any treatment initiated as dictated by the findings then a thorough history should be obtained including the time frame which the dyspnea occurred within, the severity of the dyspnea and the associated symptoms which are coexisting with the dyspnea which will provide help with narrowing down the differential list.
The time period the patient has had dyspnea is key to determining what type of diseases you should be considering in your differential diagnosis - was it sudden onset, has it developed over a few days or has it progressed over weeks or months.
- Sudden dyspnea could be caused by acute pulmonary embolism, myocardial infarction, heart valve insufficiency, pneumothorax, anaphylaxis, foreign body aspiration, pulmonary edema or cardiac tamponade. The clinician should enquire as to whether the patient has any chest pain or has had a past medical history of COPD, coronary artery disease, congestive heart failure or asthma.
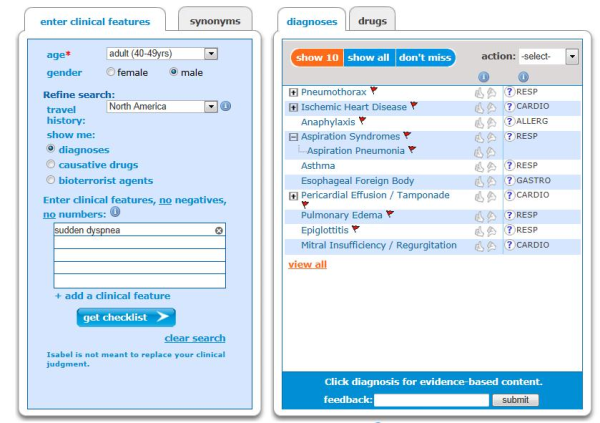
Isabel differential diagnosis for causes of sudden dyspnea – note the red flagged “Don’t miss diagnoses” which should be considered promptly and the patient worked up to rule them in or out and prevent further patient deterioration.
- Subacute dyspnea developing over hours to days could indicate acute asthma, exacerbation of COPD, pulmonary edema, myocarditis, superior vena cava syndrome, eosinophilic pneumonia or cardiac tamponade.
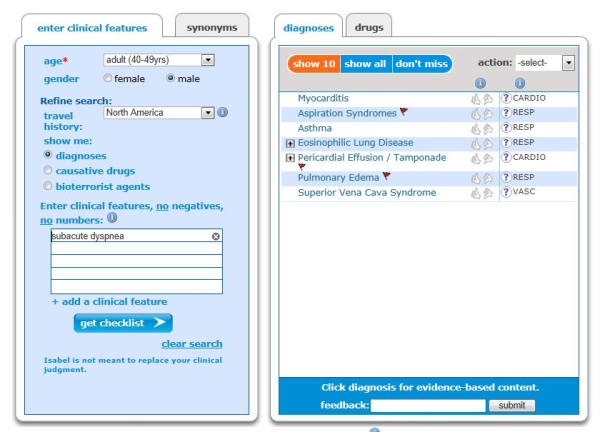
Isabel differential for subacute dyspnea which has presented over hours to a few days.
- Chronic dyspnea occurring over weeks to months may indicate COPD, congestive heart failure, idiopathic pulmonary fibrosis, pulmonary hypertension, valvular heart disease or anemia.
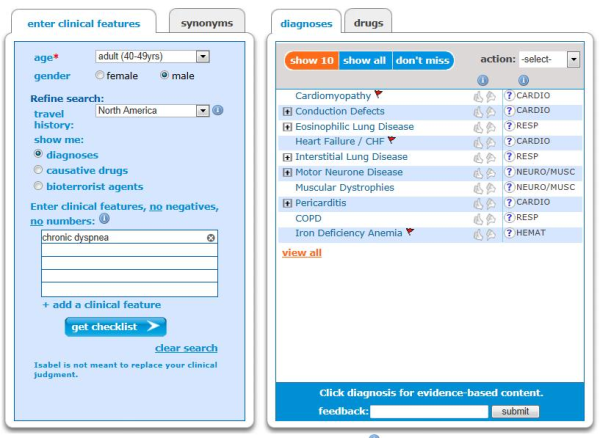
Chronic dyspnea which has manifested over a few months indicates a chronic disease which needs further investigation.
Once the patient has been examined and any findings noted, further investigation should be carried out including blood tests which include cardiac enzymes, BNP, arterial blood gases, pulse oximetry, peak flow, chest x-ray, ECG, echo and consider Holter monitoring if you suspect a cardiac cause which wasn’t detected by ECG or echo.
Dyspnea can be exhausting and frightening for the person experiencing it and providing reassurance should not be underestimated as will relieve anxiety and enable the person to concentrate on their breathing. Always ensure with a patient presenting with dyspnea that you ensure they have a secure airway and work through the “don’t miss diagnoses” to rule them in or out as a matter of urgency.
~Mandy Tomlinson, Isabel Quality Assurance Director

Mandy Tomlinson
Mandy has worked for Isabel Healthcare since 2000. Prior to this, she was a Senior Staff Nurse on the Pediatric Infectious disease ward and high dependency unit at one of London's top hospitals, St Mary’s in Paddington which is part of Imperial College Healthcare NHS Trust. Her experience in the healthcare industry for the past 33 years in both the UK and USA means she's a vital resource for our organization. Mandy currently lives and works in Scottsdale, Arizona.