




- Privacy Policy
- Terms & Conditions
- Contact us
- ©Isabel Healthcare 2025
June 20, 2019




 Dysphagia is the medical term used to describe patients who have difficulty swallowing and is common, especially in the older generation, although it can occur at any age. Each year 1 in 25 adults will experience a swallowing problem in the United States.
Dysphagia is the medical term used to describe patients who have difficulty swallowing and is common, especially in the older generation, although it can occur at any age. Each year 1 in 25 adults will experience a swallowing problem in the United States.
The normal mechanical process of deglutition, or the act of swallowing, transfers a food or liquid bolus which has been ingested and transports it from the mouth to the stomach via the esophagus. If this process is interrupted via disease or motility issues, then two types of dysphagia can occur.
Oropharyngeal dysphagia
This is a difficulty in starting to swallow and is normally neuromuscular. This means it results from dysfunction of the nerves and muscles of the mouth, pharynx at the back of the throat, or the upper esophageal sphincter muscle at the top of the esophagus. Less common than neuromuscular causes are structural causes, which can be due to strictures or tumors growing at the back of the throat. Oropharyngeal dysphagia is most common in the elderly and is normally part of other signs and symptoms that can help lead to a correct diagnosis.
Esophageal dysphagia
This occurs within the esophagus or lower down where the lower esophageal sphincter muscle connects the esophagus to the stomach. It is due to mechanical or peristaltic motility problems that obstruct the food bolus as it travels towards the stomach. Esophageal dysphagia gives a sensation of food being stuck in the neck or chest.
Taking a patient history
Taking a thorough patient history is key to identifying the cause of the dysphagia in 80% of patients. Specific questions should be framed around severity, onset and duration of the dysphagia. You should review the patient’s overall health including chronic conditions, current prescription medication, and use of alcohol and tobacco. Analyzing this information will enable you to identify if the patient is suffering from oropharyngeal dysphagia or esophageal dysphagia and whether the cause is neuromuscular or obstructive.
Symptoms of dysphagia
General symptoms indicating dysphagia include:
- being unable to swallow
- odynophagia (pain on swallowing)
- drooling
- hoarseness
- choking when eating
- regurgitation of food
- frequent heartburn
- weight loss
- coughing when swallowing
- cutting food into smaller pieces
- gagging when swallowing
- recurrent pneumonia due to aspiration when eating or drinking
- change in speech
- nasal regurgitation
In oropharyngeal dysphagia the patient will have difficulty initiating swallowing and may also experience coughing, choking and nasal regurgitation. When the patient speaks, they may have a nasal tone.
In esophageal dysphagia the patient will have the sensation of food being stuck in their throat or chest.
In any dysphagia whereby the origin is neuromuscular, the patient will experience progressive difficulty swallowing solid food and liquids. The food bolus may be helped to pass by repeatedly swallowing, raising the arms, throwing the shoulders back or changing position. Performing the Valsalva maneuver will also provide relief. These patients are more likely to experience pain on swallowing.
Mechanical obstruction is associated with solid food dysphagia but not liquids. Again, the Valsalva maneuver may help with the passage of the food bolus but the patient may also regurgitate undigested food or vomit. Enquire about diet changes as it may be found the patient has switched to soft foods as they find them easier to swallow. Weight loss will tend to be found if the cause of the dysphagia is mechanical obstruction.
Physical Examination
A neurological evaluation should be performed assessing mental status, deep tendon reflexes, cranial nerve and cerebellar examination.
Observe the patient eating and drinking and assess their mechanics of swallowing and also if they produce enough saliva to form a bolus with the food.
Differential diagnosis of dysphagia
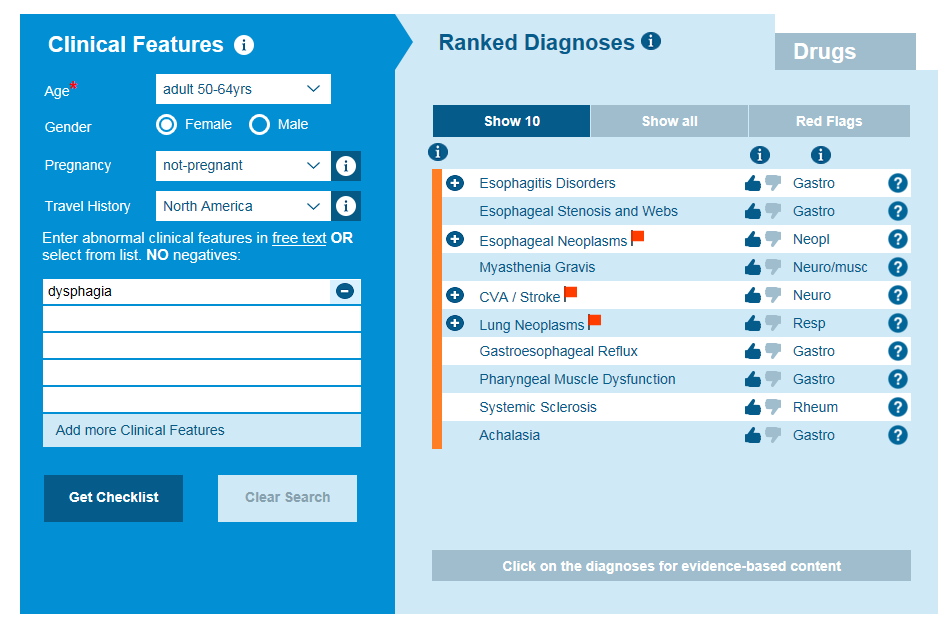
Isabel differential diagnosis of dysphagia
At this point after conducting a history, a physical examination, and identifying the patient’s symptoms, you should be able to form a differential diagnosis for dysphagia. If you are uncertain of the causes then Isabel can assist you at this point, with information that will also help you refine your differential and identify whether the origins of the dysphagia are oropharyngeal or esophageal, as well as whether the cause is neuromuscular or obstructional.
Oropharyngeal dysphagia causes include:
- neurological disorders stemming from multiple sclerosis, muscular dystrophy or Parkinson’s disease
- Strokes, brain injuries, or spinal injuries, that have caused neurological damage
- Tumors and certain cancers.
Esophageal dysphagia can be caused by:
- Strictures or obstructions of the esophagus. This can be due to tumors, scar tissue (caused by gastroesophageal reflux disease) or foreign bodies
- Tumors of the alimentary tract or chest growths, compressing the esophagus
- Eosinophilic esophagitis, which is an overpopulation of eosinophils in the esophagus and may be caused by a food allergy
- Achalasia, a condition where the lower esophageal sphincter muscle doesn’t relax and let food into the stomach. There may be poor peristaltic movement in the esophagus, so food/liquid is regurgitated into the throat.
When the differential diagnosis has been formed you can then decide what studies to perform to make the diagnosis depending on where the dysphagia is oropharyngeal or esophageal and whether the cause is determined to be neuromuscular or obstructive. Studies include endoscopy, barium studies, video radiographics, pH monitoring, and nasopharyngoscopes, which will enable you to make the final diagnosis.
Dysphagia severely impacts a patient’s quality of life and if not diagnosed and treated early then complications of malnutrition, weight loss and dehydration can occur as the patient is unable to maintain an adequate fluid and diet intake. Aspiration pneumonia is a complication of dysphagia as food and liquid enters the airway when the patient swallows, which allows the food to introduce bacteria into the lungs. Identifying recurrent pneumonia in these patients will assist with confirming the patient has dysphagia and looking for a cause. Choking occurs in patients when their airway is partially or fully blocked and if not remedied can cause loss of life. For these reasons dysphagia needs to be worked up promptly and comprehensively in order to arrive at a diagnosis and treat the patient accordingly.
Interested about what Isabel can do for you or your institution? Take our 30 day free trial and see the power of the Isabel DDx Generator.

Mandy Tomlinson
Mandy has worked for Isabel Healthcare since 2000. Prior to this, she was a Senior Staff Nurse on the Pediatric Infectious disease ward and high dependency unit at one of London's top hospitals, St Mary’s in Paddington which is part of Imperial College Healthcare NHS Trust. Her experience in the healthcare industry for the past 33 years in both the UK and USA means she's a vital resource for our organization. Mandy currently lives and works in Scottsdale, Arizona.