




- Privacy Policy
- Terms & Conditions
- Contact us
- ©Isabel Healthcare 2025
May 15, 2012




Necrotizing Fasciitis – "Don’t miss" as patient can quickly be severely harmed. Diagnosis is physical: Necrotizing fasciitis is an uncommon but life-threatening condition that carries a high risk of mortality and associated complications. It requires a high index of suspicion in order for it to be correctly diagnosed. Organisms invade a wound site and spread along the superficial and deep fascial planes causing a necrotizing infection. Necrotizing fasciitis should be urgently considered in any patient presenting with:
- a soft tissue infection or wound
- prominent pain or numbness over the infected area
and/or
- sepsis including tachycardia, hypotension and fever.
Necrotizing fasciitis infections can be classified into these types:
Type 1 – polymicrobial infection consisting of aerobic and anaerobic bacteria (Bacteroides,Peptostreptococcus, Eschericia coli, Klebisella) that is usually seen in immunocompromised patients or those with chronic disease.
Type 2 – is a monomicrobial infection of streptococus infection caused by group A steptococcus which can occasionally present with a staphylococcal infection. It can also be caused by vibrio vulnificus and aeromonas hydrophila which are marine organisms and can enter a wound following seawater contamination of wounds. These marine organisms are quite virulent and can be fatal or cause devastating consequences if not picked up quickly.
Risk factors to be considered when diagnosing Necrotizing fasciitis include:
- Varicella zoster infection - the lesions allow organisms to enter the body
- Traumatic (cut, wound) or nontraumatic cutaneous lesion (eczema, psoriasis, skin ulcer which allows entry for the bacteria
- Intravenous drug use leaves a puncture mark where organisms can break through
Key symptoms to look out for are:
- cutaneous lesion
- severe pain over site of wound or cellulitis – it should be noted that the pain experienced by the person may be disproportionate to the visible skin changes. Necrotizing fasciitis can occur in the extremities, perineum, trunk, head, neck and abdominal areas.
- fever
- palpitations
- dizziness
- hypotension
- nausea
- vomiting
- delirium
Have a high suspicion for Necrotizing fasciitis if the patient has encountered any of the following:
- Unexplained limb pain
- Systemically ill with severe pain
- Enquire about recent illness, exposure to sea water, fish stings or intraveous drug abuse
As this is a rapid developing infection, if necrotizing fasciitis is suspected then surgical exploration and debridement is needed along with administering broad spectrum antibiotics as the diagnosis is clinical. Further tests on CBC, CRP etc. can be carried out as time allows but visualisation of the tissues during surgery will show a necrotizing soft tissue infection which is diagnostic of this disease.
Using a diagnosis checklist system like Isabel will alert clinicians to consider these urgent don’t miss diagnoses and to positively rule them in or out of their differential diagnosis or ddx checklists to ensure the best outcome for their patients. Necrotizing fasciitis has to be treated quickly to prevent death and other complications like loss of limbs or damage to the body and its organs.
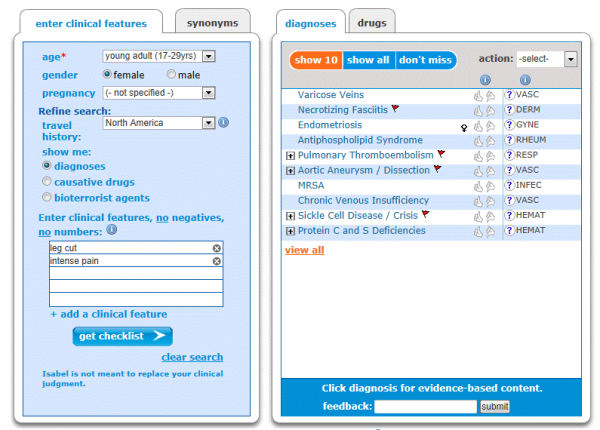
Isabel decision support showing red flagged don’t miss diagnosis of Necrotizing fasciitis for a patient presenting with a leg cut associated with intense pain
~Mandy Tomlinson, Isabel Quality Assurance Director
Mandy Tomlinson
Mandy has worked for Isabel Healthcare since 2000. Prior to this, she was a Senior Staff Nurse on the Pediatric Infectious disease ward and high dependency unit at one of London's top hospitals, St Mary’s in Paddington which is part of Imperial College Healthcare NHS Trust. Her experience in the healthcare industry for the past 33 years in both the UK and USA means she's a vital resource for our organization. Mandy currently lives and works in Scottsdale, Arizona.